


If you’re struggling to think of something positive to come out of this pandemic, let me suggest the ability to adapt to and overcome the challenges and changes that have been forced upon primary care. We’ve had to deal with ever-moving goalposts, changes to routines, the hurry up and wait for clear and concise direction. Yet, team cohesion, a can-do attitude and great leadership within practices have ensured that our patients have been given an excellent level of service at all times.
So, if we can adapt to change, what has this shown the CQC? Well, it’s shown them that they also need to adapt to change and make changes to their approach to regulation… Yes, I know they’ve changed their approach already as we’ve experienced the ERS, TMA and TRA, and now there’s further change planned. But what will it mean for you? What do the CQC want to do differently? Take a look at this news released on 26th January to learn more.
Comprehensive inspections
There’s an aspiration to step away from on-site, comprehensive inspections. Instead, the approach taken by the CQC will be to use various sources of evidence to assess quality. This doesn’t mean this is the end of the on-site inspection; but, very much like the CQC have done during the pandemic, if there’s deemed to be a risk to patient safety, an on-site inspection will be carried out.
The plan is to use the information they have and gather to update ratings. If further information is required for them to be able to do this, then the requests will be relevant to the information sought. Who’d have thought it: an assessment and rating without visiting the premises! Is this the right way to go? Does this give organisations the opportunity to ‘bluff’ their way through an inspection? Should there continue to be site visits? I’m sure there will be mixed responses. While site visits are time-consuming and, for some, stressful experiences, isn’t that approach needed? And what better way to regulate than to visit the practice and engage with patients and the team? In my opinion (my views are my own), I do believe we need site visits (just saying). After all, it provides the regulator with assurances that service delivery is safe, effective, caring, responsive and well led.
Now that I’ve probably lit the blue touch paper, I’ll move on.
Ratings
In my naval career, the word ‘ratings’ had a totally different meaning: ‘A rating of the lower deck’ was anyone below officer rank. Anyway, before I go into Uncle Albert mode, I’ll crack on! More flexibility is suggested when it comes to updating ratings and, interestingly, there are changes afoot regarding inspection frequencies too.
The intended approach will be to review, confirm and change ratings using the best available information about quality, taking into consideration patients’ experiences and feedback, national and local insight data and through self-assurance. The objective is to reflect changes in ratings more quickly. As I mentioned earlier, the CQC want the flexibility to adopt a risk-based approach.
The CQC admit the current approach to regulating GP practices is too complex. So, what do the CQC suggest? A two-level rating for GP practices, as follows:
Level 1: A rating for each key question for the location/service. This will be based on relevant evidence of how GP practices personalise people’s care and provide care for different groups of people.
Level 2: An overall rating for the service. This will be an aggregated rating informed by their finding at Level 1.
Have a look at the example below to see how the simplified ratings could look:
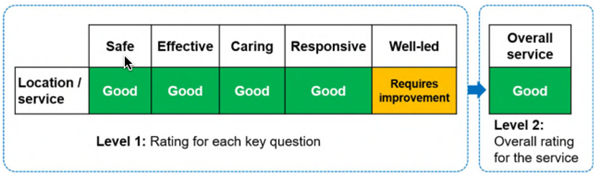
Image source: cqc.org.uk
Is this a positive step forward? What this does mean is that the CQC won’t provide a separate rating for different groups of people for the effective and responsive key questions. Do you think this approach will have an impact on patient care? If so, will this be a positive or negative impact? One thing is for sure, the CQC won’t stop looking at how providers offer personalised and proactive care.
What do you think?
How do you feel about the suggested changes? Do you have concerns, or will you welcome such changes? Changes are (in my opinion) needed. There has to be flexibility, there have to be smarter ways of working, a more streamlined approach to the (dare I say it) inspection process. At the end of the day, the regulator has to be assured that patient safety isn’t being compromised. Wouldn’t a site visit be necessary? After all, you can’t determine the safety of a vehicle by carrying out an MOT remotely. Nor can you assure yourself that your child’s school is ‘good’ if OFSTED haven’t visited!
If you want to have your say regarding the proposed changes, you can do so by responding to the CQC online, using this link.



0 Comments